PLANTAR FASCIITIS
Heel pain is a common presenting complaint in the foot and ankle. Plantar Fasciitis (PF) is the most common cause of chronic pain beneath the heel in adults. This makes up 11–15% of the foot symptoms requiring professional care among adults. Estimates say that 1 in 10 people will develop PF during their lifetime. PF, which is more common in middle-aged higher-weight females and young male athletes, has a higher incidence in the athletic population though not all suffering require medical treatment. PF’s symptoms are:
– painful heel syndrome
– chronic plantar heel pain
– heel spur syndrome
– runner’s heel, and
– calcaneal periostitis.
There are some factors associated with PF will help identifying at risk individuals and development of new and improved preventative and treatment strategies. Obesity is present in up to 70% of patients with PF. There is a strong association between increased body mass index (BMI) and PF in a non-athletic population. The evidence suggests that unlike weight, height has no association with PF. More specifically, increased weight is associated with PF, but not necessarily with reduced height.
Heel spurs are a risk factor for PF. Current studies demonstrate a highly significant association between calcaneal spur and PF. There are also deficits in flexibility of the plantar flexor muscles may contribute to a greater fascia stretching. Some reports suggest that 81–86% of patients with PF have excessive pronation. Despite the fact that the pronated foot posture and over-pronation during gait are commonly cited as causative factors for PF, there is conflicting evidence with regard to the association of static foot posture and dynamic foot motion with PF.
Clinical features and diagnosis
The diagnosis of PF is usually clinical and rarely needs to be investigated further. The patient complains of pain in the medial side of the heel, most noticeable with initial steps after a period of inactivity and usually lessens with increasing level of activity during the day, but will tend to worsen toward the end of the day.
Symptoms may become worse following prolonged weight bearing, and often precipitated by increase in weight bearing activities. Paresthesia is uncommon. PF is usually unilateral, but up to 30% of cases have a bilateral presentation. Tightness of Achilles tendon presents in almost 80% of cases.
Occasionally the pain may spread to the whole of the foot including the toes. Tenderness can be elicited over the medial calcaneal tuberosity and may exaggerate on dorsiflexion of the toes or standing tip toe.
PLANTAR DIAGNOSIS
Imaging studies are typically not necessary for diagnosis of PF. In the clinical management of chronic heel pain, diagnostic imaging can provide objective information. This information can be particularly useful in cases that do not respond to first-line interventions, or when considering more invasive treatments (e.g. corticosteroid injection).
Lateral radiograph of the ankle should be the first imaging study. It is a good modality for assessment of heel spur, thickness of plantar fascia, and the quality of fat pad. Plain radiography identifies stress fractures, unicameral bone cysts, and giant cell tumors usually.
Ultrasound examination is operator-dependent, but it proves to be significant when the diagnosis is unclear.
Plantar fascia thickness values have also been used to measure the effect of treatments and there is a significant correlation between decreased plantar fascia thickness and improvement in symptoms. MRI can be used in questionable cases, which fail conservative management or are suspected of other causes of heel pain, such as tarsal tunnel syndrome, soft tissue and bone tumors, osteomyelitis, subtalar arthritis, and stress fracture.
PLANTAR TREATMENT
Numerous interventions are available for treatment of PF. The predominant ones include: rest, heat, ice pack, non-steroidal anti-inflammatory drugs (NSAIDS), heel pads, magnetic insole, night splints, walking cast, taping, plantar and Achilles stretching, ultrasound, steroid injection, extra-corporeal shock wave therapy, platelet-rich plasma injection, pulsed radiofrequency electromagnetic field therapy, and surgery.
Stretching
Stretching may be in calf or plantar region. Numerous authors recommend calf stretching as one of the interventions for patients with PF. A calf stretch is one where the patient stands with staggered legs facing toward a wall, with both hands stretched out.
Night splints
The design of night splinting is to keep the patient’s ankle in a neutral position overnight, passively stretching the calf and plantar fascia during sleep. There is no difference between the various types of the night splints whose purpose is to allow the fascia to heal.
Surgery
Recalcitrant cases where symptoms persist for more than 6–12 months, even after adequate conservative treatment are usually cases for surgery. Before surgery, consideration is given to nerve conduction and electromyographic studies to determine compression of the posterior tibial nerve.
Immediate Help through Physiotherapy for Plantar Fasciitis:
Have you been experiencing aching pain in the heel? Looking for orthotics for Plantar Fasciitis? Wondering if the symptoms that you are experiencing are of Achilles Plantar Fasciitis? Wanting to learn physio stretches for Plantar Fasciitis? Interested in trying out the benefits of physio laser approach for heel pain?
At Curezone Physiotherapy, our expert therapists aim to relieve you of heel pain through various physio stretching manoeuvres and customized heel pain exercises. If you are looking for the best physio NEAR ME to learn the exercises to eliminate heel pain, look no further! Our aim is to be YOUR best physiotherapist in Mississauga and Oakville areas, and are here and ready to teach you the best exercises for the physical injury causing heel pain. We are a physiotherapy covered by OHIP.
We welcome you to call us or click below to book an appointment with one of our expert physiotherapists to let us immediately start assisting you in your road to recovery.
Physio for Plantar Fasciitis, Mississauga:
Physiotherapy Clinic Mississauga – Curezone Physiotherapy, Heartland Mississauga.
Physiotherapy Clinic Erin Mills – Curezone Physiotherapy, Erin Mills Mississauga.
Physio for Plantar Fasciitis, Oakville:
Physiotherapy Clinic Oakville – Curezone Physiotherapy, Burloak Oakville.

Hip PAIN, HIP Joint Injuries, and Physiotherapy
Hip Joint Injuries and physiotherapy - Curezone Physiotherapy
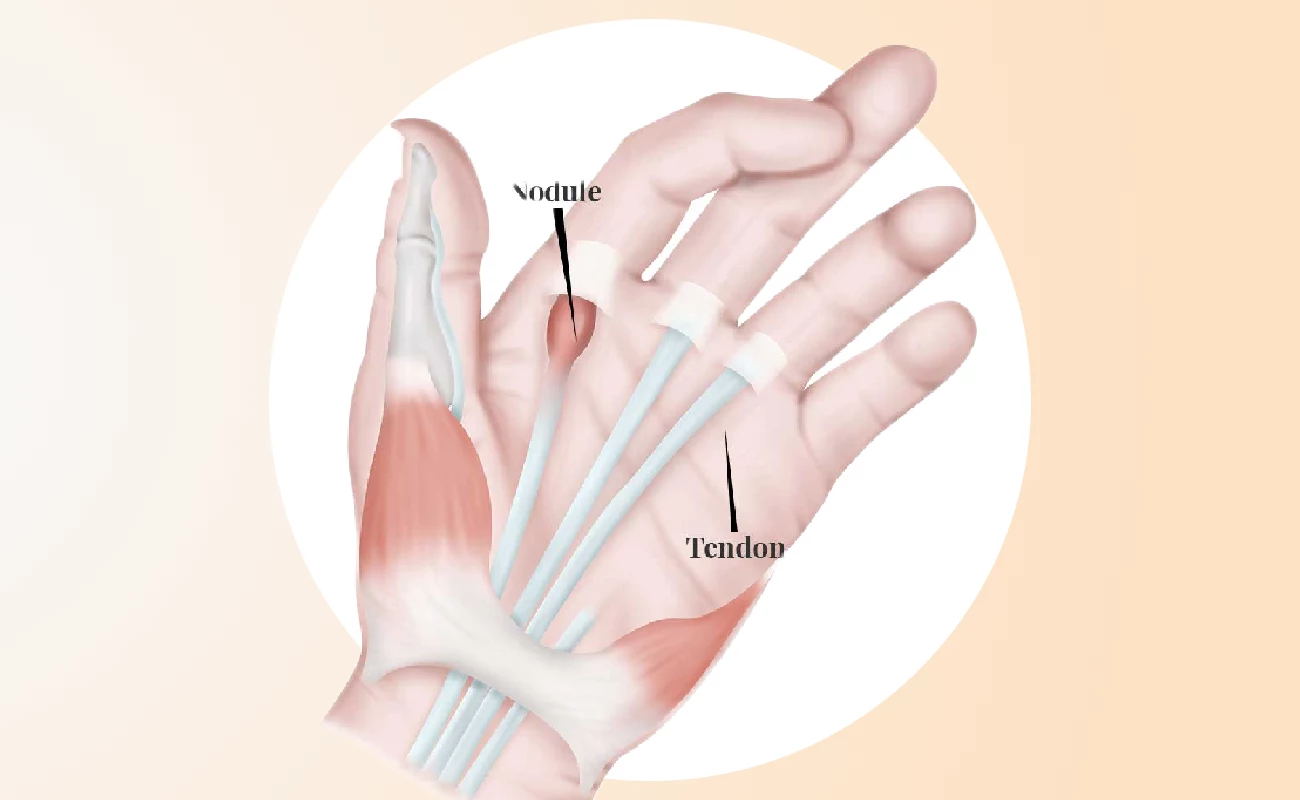
Trigger Finger hand exercises Physiotherapy
Hand Exercises Looking for exercises to treat Trigger Finger? Our physiotherapy in Mississauga offer

Hamstring Strain Buttock Pain Physiotherapy Treatment
Hamstring injuries are common in athletes and become a troublesome chronic condition. The hamstring