
Anatomy of the Knee Joint
The knee joint is a very complex joint due to the many ligaments in and around the knee as well as the muscles and bones that surround the structure. The femur connects to the tibia (shin bone) where they meet the knee joint. Anterior to the structure of the knee joint is the patella, a small sesamoid bone. Lateral to the tibia is the fibula. In this structure you will find many ligaments and tendons of muscles that support the knee joint as well as mobilize it. Sitting on top of the Tibia there are two C-shaped discs known as the Menisci; the lateral menisci and the medial menisci. The role of both of these menisci is to absorb shock by dissipating forces out and deepening the tibia articulation increasing joint stability.
The medial meniscus is attached to the medial collateral ligament (MCL) and the joint capsule. If there was ever damage to the MCL it is possible that the medial meniscus is torn. The lateral meniscus is smaller and does not have extra attachments; it is just attached to the tibia. Around any joint you will most likely find these fluid filled sacs known as bursae which help reduce wear and tear on the joint. In the knee joint there are 4 bursae which help lubricate the knee so it can reduce tearing.
There are 4 movements of the knee joint those being knee Extension an action produced by the quadriceps tendon, Flexion an action made by the hamstrings, gracilis, sartorius and the popliteus, Lateral Rotation an action produced by one of the hamstring muscles; the biceps femoris, and finally Medial Rotation an action produced 2/3 hamstring muscles that include semimembranosus, semitendinosus it also includes other muscles like gracilis, sartorius and popliteus.
Ligaments
Patellar Ligament; this is a continuation of the quadriceps tendon which attaches to the tibial tuberosity.
The Collateral Ligaments
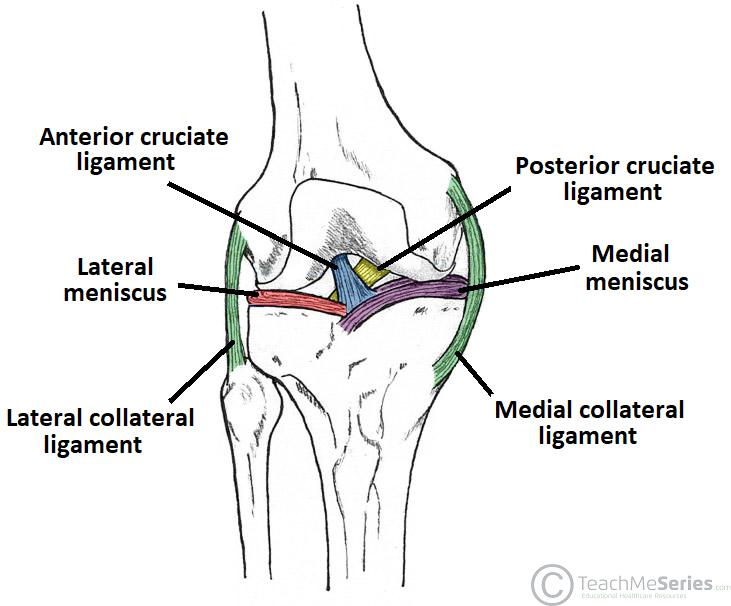
Medial Collateral Ligament (MCL): which is found on the medial side (close to the midline) of the knee joint it attaches at the medial epicondyle of the femur and to the medial condyle of the tibia.
The Lateral Collateral Ligament (LCL): found on the lateral side of the knee joint attaches to the lateral condyle of the femur and the lateral surface of the head of the fibula.
The Cruciate Ligaments which connect the femur and the tibia and they cross over each other hence the word cruciate.
The Anterior Cruciate Ligament (ACL): attaches at the anterior aspect of the tibia and blends in with the medial meniscus. It ascends posteriorly and attaches to the femur; this ligament prevents an anterior sliding of the tibia on the femur.
The Posterior Cruciate Ligament (PCL): attaches at the posterior aspect of the tibia and ascends anterior to attach at the medial femoral condyle. This ligament prevents posterior dislocation of the tibia on the femur.
Injuries
Collateral Ligaments are most commonly injured these are the MCL and LCL it is caused by either a varus or valgus force applied to either side of the knee while the foot is planted on the ground. To confirm where the pain is you will be asked to medially or laterally rotate the leg if there is pain on the medial rotation there is an injury to the MCL if there is pain on lateral rotation there is an injury to the LCL. If the MCL is severely damaged with a grade three sprain or a full rupture there is a possibility that the medial meniscus can be torn.
Cruciate Ligaments: The ACL is torn when the knee becomes hyperextended or when there is a large force to the back of the knee driving the femur anteriorly on the tibia while the knee joint is slightly flexed. To test this the physiotherapist will perform the anterior drawer test when the knee is flexed and the therapist pulls the tibia anteriorly, if the ligament moves it can possibly be torn. The PCL is torn when the knee is flexed and a large force is on the shins pushing the tibia backwards. This injury is common in motor vehicle accidents (MVA) when the knee and lower leg hit the dashboard. To test if this ligament is injured a physiotherapist will perform the posterior drawer test when the knee is flexed and they push the tibia posteriorly if there is any movement the ligament can be torn. It is important to note that some people have lax ligaments so if this test is done on you and there is a slight movement with no pain it does not mean the ligament is torn.
The Unhappy Triad is a common term used in sports when the ligaments of the knee have been injured, more specifically the MCL, Medial Meniscus and the ACL. This happens when a lateral force is applied to the knee while in extension for example getting hit on the outside of the knee in football that ruptures the MCL, damages the medial meniscus and also damages the ACL hence the unhappy triad.
Strengthening the Knee Joint
Strengthening the knee joint is very important after an injury. The muscles that you should focus on strengthening that will stabilize and improve function of the knee joint are the hamstrings, quadriceps, glutes and hip muscles (hip adductors and flexors).
Starting with stretches
- Lying hamstring stretches (lie on back and lift leg to the sky and pull closer to the body until stretch is felt)
- Figure 4 Stretch
- Standing hamstring stretches
- Standing Quad stretch
- Lateral Lunges
Exercises
- Squats (These can be modified, regressed and progressed based on the patient)
- Seated Leg Raises or Seated Knee Extensors (Can use resistance bands or any other resistance equipment)
- Hamstring Curls
- Single Leg dips with support
- Step Ups (Choose Different box heights making the step harder to climb)

Physiotherapy for Sacroiliac Joint Dysfunction
Physiotherapy for Sacroiliac Joint Dysfunctions

Thoracic Outlet Syndrome
The term ‘thoracic outlet syndrome’ describes compression of the neurovascular structures as the

Tennis Elbow Physiotherapy
Get relief from tennis elbow with effective physiotherapy treatment specifically designed to target